Case 4
This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
September 21, 2021
Date of Admission-18-9-21
A 29 years old female presented to OPD with chief complaints of fever, cough, cold since 5 days.
HISTORY OF PRESENT ILLNESS
Patient was apparently well 5 days back.
Patient complaints of generalised weakness, dizziness since 5 days and shortness of breath, sweating since 2 days.
No history of dysphagia, loss of appetite, hypothyroidism, weight loss
HISTORY OF PAST ILLNESS
Patient has history of gall bladder stone 6 years back undergone surgery.
Patient has history of uterus intramural fibroid at posterior upper body and fundamental part which was detected on USG 4 months back.
Patient was detected with minimal free fluid in post operative delirium region which suggests pelvic inflammatory disease 4 months back.
Patient was detected with grade 1 and grade 2 fatty liver.
No history of hypertension, CAD, tuberculosis, asthma.
PERSONAL HISTORY
Diet- mixed
Appetite-normal
Sleep-adequate
Bowel and bladder movement-regular
No addictions
FAMILY HISTORY
Patient complaint that her father is hypertensive.
TREATMENT HISTORY
Patient consumes metformin 500mg twice daily since 2 years.
MENSTRUAL HISTORY
Patient has 30 days cycle with regular flow for 4 days.
Maternal status-Patient got married at the the age of 14 and has 3 children.
GENRAL EXAMINATION
Patient is conscious,coherent, co-operative and well oriented to time and place
There is no sign of pallor,oedema of left foot
There is no sign of cynosis,lymphadenopathy.
VITALS
Temperature-94.6 degree F
Pulse rate-103 per min
Respiratory rate-38 per min
Spo2-98

SYSTEMIC EXAMINATION
Cardiovascular System
Thrills-No
Cardiac sound-S1 and S2
Cardiac murmers-No
Respiratory System
Dysnoea-No
Wheeze-No
Position of trachea-central
Breathe sound-vesicular
Abdomen
Shape-scaphoid
Tenderness-No
Palpable mass-No
Free fluid-No
Bruits-No
Liver and spleen-not palpable
Bowel sounds-No
Central Nervous System
Patient is conscious
Speech-normal
Meningitis irritation-No
PROVISIONAL DIAGNOSIS
Pyrexia decreased evaluation with diabetes mellitus type 2
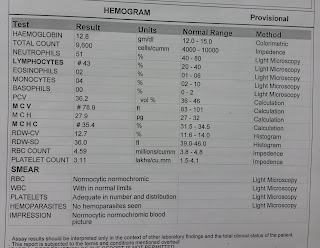
INVESTIGATION







TREATMENT
Day 1
IV FLUIDS:
Normal saline @100mL/L
Ringer lactate solution@ 100mL/L
Tab.PCM 650mg PO/SOS
Inj.OPTINEURON 1amp in normal saline @100 mL/L
Inj.PAN 40 mg/PO/OP
Blood pressure , pulse rate , SpO2 monitoring.
Tab.GLIMI -M1PO/OD.
Day 2
IV FLUIDS:
Normal saline @100mL/L
Ringer lactate solution@ 100mL/L
Tab.PCM 650mg PO/SOS
Inj.OPTINEURON 1amp in normal saline @100 mL/L
Inj.PAN 40 mg/PO/OP
Blood pressure , pulse rate , SpO2 monitoring.
Tab.GLIMI -M1PO/OD.
Tab.Levocetrizine 5mg/PO/HS.
Tab.Clonazepam 0.25mg/PO/HS.
Day 3
IV FLUIDS:
Normal saline @100mL/L
Ringer lactate solution@ 100mL/L
Tab.PCM 650mg PO/SOS
Inj.OPTINEURON 1amp in normal saline @100 mL/L
Inj.PAN 40 mg/PO/OP
Blood pressure , pulse rate , SpO2 monitoring.
Tab.GLIMI -M1 PO/OD.
Tab.Levocetrizine 5mg/PO/HS.
Tab.Clonazepam 0.25mg/PO/HS.
What is Pyrexia?
Pyrexia is grouping of many unrelated medical condition that share the feature of persistent unexplained fever despite basic investigation.
Main stages of the molecular basis of pyrexia-:

Causes of Pyrexia- bacterial infection, viral infection, malignancy, autoimmune
Pathophysiology of diabetes mellitus and infections-:




Comments
Post a Comment